In the early part of the pandemic, many people charted the emerging picture of high Covid-19 death rates in developed countries with a large pharmaceutical industry presence (whose governments generally opposed HCQ) and low rates in poorer countries (that already used HCQ or were quick to adopt it).
This resulted in a number of comparative analyses.
Summary
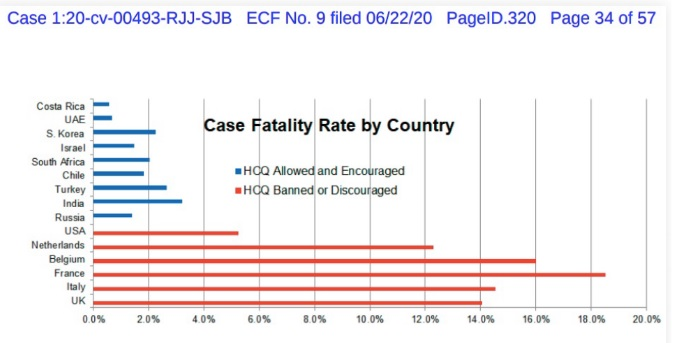
(i) An analysis by the group Americas Frontline Doctors by country, showed that access to HCQ was strongly linked to lower Covid-19 mortality.
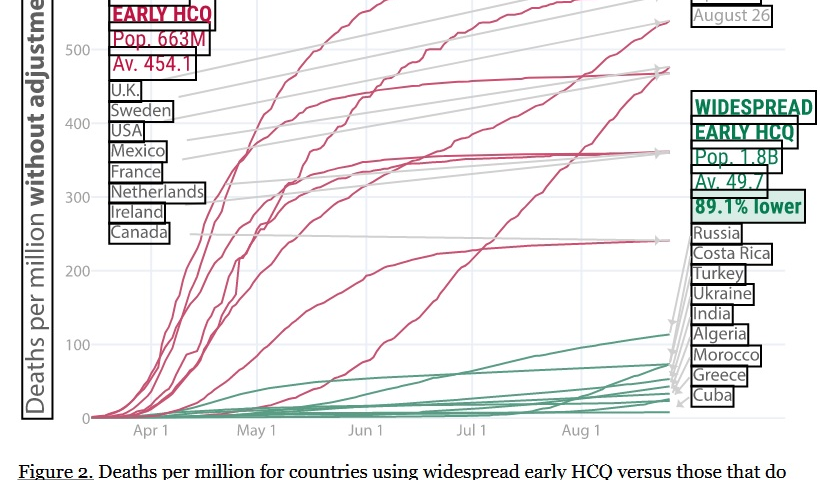
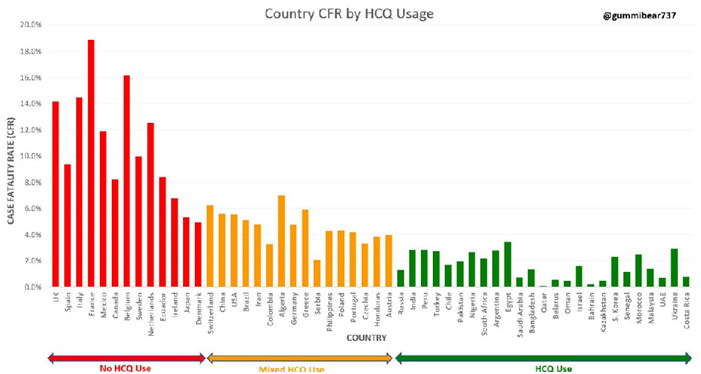
(ii) A worldwide country comparison generated automatically by the website C19study.com showed that countries with widespread use of HCQ had much lower death rates than those with limited or no HCQ use.
(iii) A study by Izoulet found that countries using antimalarial drugs HCQ and CQ (chloroquine) fared better than those which did not.
(iv) Elbazidi and Erraih found a strong negative correlation between President Trump’s approval ratings (which they related to HCQ use) within US states and the states’ Covid-19 Case Fatality Rates.
(v) In a support analysis of HCQ decisions from other countries, they also found a very strong correlation between the issue dates of HCQ directives and the dates of change in the evolution trend of the fatality rate.
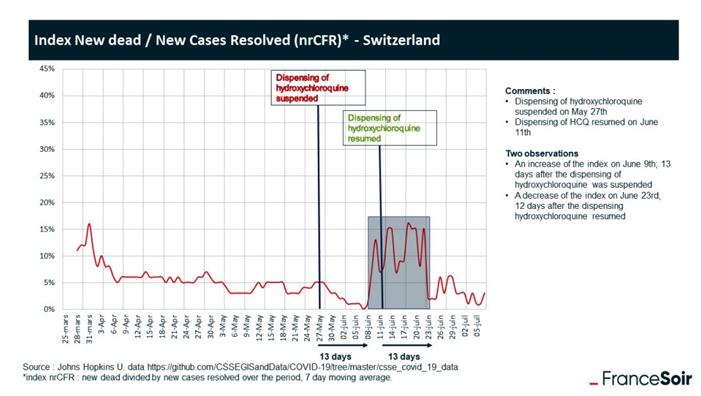
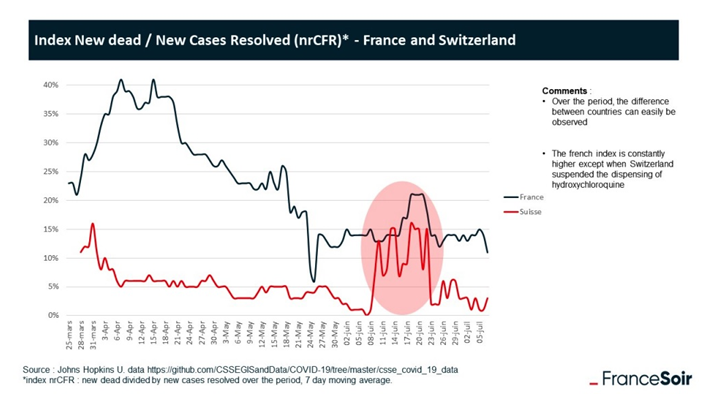
(vi) An inadvertent experiment. A period where HCQ was halted and then restarted in Switzerland and France resulted in the Covid-19 death rates in those two countries rising and then falling compellingly.
These studies highlighted and quantified what those who had been observing the emerging data had already observed for themselves.
(vii) Another Cross-Country Analysis (Toya and Skidmore, April 2021) found that “that countries with greater income, less dense and greater elderly populations, fewer hospital beds, and more freedom experienced greater fatalities, and that travel restrictions and use of hydroxychloroquine reduced deaths.”
The authors noted that according to their regression estimate, “if the U.S. had made HCQ widely available, fatalities would have been reduced from about 515,000 to 427,000“, and that “HCQ use is perhaps the most effective low-cost policy option for reducing fatalities.”
Details
(i) In their White Paper on Hydroxychloroquine, AFD wrote:
“Country by country data is also available and access to HCQ is strongly linked to lower mortality.77 We can see that even very poor countries have much lower case fatality rates than wealthy countries, which of course, is typically the opposite of what we would expect of a respiratory disease that could end up in an ICU admission. Kazakhstan, Bangladesh, Senegal, Pakistan, Serbia, Nigeria, Turkey, Ukraine, Honduras … the list goes on. Wealthier democracies or countries with especially abusive HCQ protocols such as are doing terribly: Ireland, Canada, Spain, The Netherlands, UK, Belgium, France … Of note, Italy and Spain switched mid-stream and now HCQ is easily available.”
A sample graph was given. The data can be viewed here
(ii) A worldwide country comparison
The largest country comparison was carried out by the C19study group who found that countries with widespread use of HCQ had much lower death rates than those with limited use. A compelling graph to this effect, like the one below, was widely circulated.
However it was also part of a lengthy report. The analysis from C19study was endorsed by Dr Raman Oskoui, a fellow of the American College of Cardiology. Fox News, Aug 7, 2020. Speaking with host Laura Ingraham:
Massive International Study Shows Countries with Early HCQ Use Had 79% Lower Mortality Rate
Dr Oskoui said:
“I think this data is legitimate, they provide over 150 references to support their findings. The data is really damning; what you see is that countries that don’t spend like we do, like don’t spend 20% of their GDP on health care, have done incredibly well with Covid, and it’s really devastating to Dr Fauci, … Dr Redfield in their performance; not only should they be embarrassed, but i think they really need to be held to account“.
(iii) Countries which Primarily Use Antimalarial Drugs As COVID-19 Treatment See Slower Dynamic of Daily Deaths ( Izoulet, 28/5/20). In short, Izoulet found a striking difference.

(iv) and (v) Elbazidi and Erraih, July 2020 featured two GCQ analyses by country/state:
In (iv) Trump’s approval rating (which according to the authors was strongly linked to acceptance of HCQ-based treatment in the states) was negatively strongly correlated with states’ Covid-19 case fatality rates (CFR).
In the country analysis (v) the authors compared 6 countries that made clear-cut decisions (for or against) regarding the use of HCQ. They found the ranks or ordering of the dates of the HCQ decisions correlated with the delay of trend changes of the CFR evolutions for these 6 countries
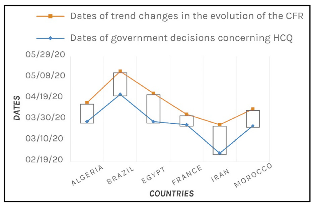
and inferred:
“the use of HCQ on the whole population of a country affects directly the evolution of the CFR of that country“
Another widely spreadgraph from the C19study group data was this one:
(vi) The inadvertent experiment
The appearance of the fake Lancet anti-HCQ study caused HCQ to be temporarily banned in Switzerland for two weeks, soon being restored there when the study was hastily retracted under a cloud of suspicion.
This created an unusual opportunity to examine start-stop HCQ data.
Analysis by the French newspaper FranceSoir showed that the graph of Swiss Covid-19 deaths at this time, after a short lag took a sharp rise and fell steeply after two weeks, as if in step.
A quantitative test put the probability of this happening purely by chance, to the extent that it did, at less than 0.001.
The data from France, which also halted HCQ at this time, exhibited the same pattern:
https://www.francesoir.fr/societe-sante/covid-19-hydroxychloroquine-works-irrefutable-proof
See also here
This challenge-dechallenge-rechallenge is along the lines of the classic Bradford-Hill criteria for assessing causality [1].
It is one of the standard methods of assessing causality in France [2].
And, indeed, Switzerland [3]
[1] FDA blog: ” Causation is almost always considered more likely when a positive (+) re challenge exists. Review of this information falls under experimental evidence within Bradford Hill’s criteria.1
[2] 1 Hill AB. The Environment and Disease: Association or Causation? Proc R Soc Med” https://biotechresearchgroup.com/epidemiology-topics-population-dechallenge
Also see https://journals.sagepub.com/doi/10.1177/009286158401800314
[3] Causality assessment criteria, https://smw.ch/article/doi/smw.2021.20400
Finally, the following snippet, from material presented to a US court, was a damning indictment of the FDA policy of suppressing both a life-saving drug and the expertise of physicians:
ASSOCIATION OF AMERICAN PHYSICIANS & SURGEONS v FDA